Cryopreservation is freezing tissue or cells in order to preserve it for the future.
- Cryopreservation is used in infertility programs to freeze and store sperm, eggs or to freeze “leftover” embryos from an in vitro fertilization cycle
- There are 2 methods currently used for freezing in IVF labs
- Slow freezing
- Vitrification (ultra-rapid freezing)
- Our IVF program has been using vitrification to freeze leftover embryos since 2008 – we see excellent success rates with frozen embryo transfer cycles
What percent of patients will have excess embryos for freezing?
The response to ovarian stimulation and egg quality are both age-dependent. Therefore, the percent of couples with embryo freezing varies based on female age.
- The graph below shows the percentage of IVF egg retrievals in our program that had leftover embryos frozen in 2010-2011
- Note the significant decrease with advancing female age
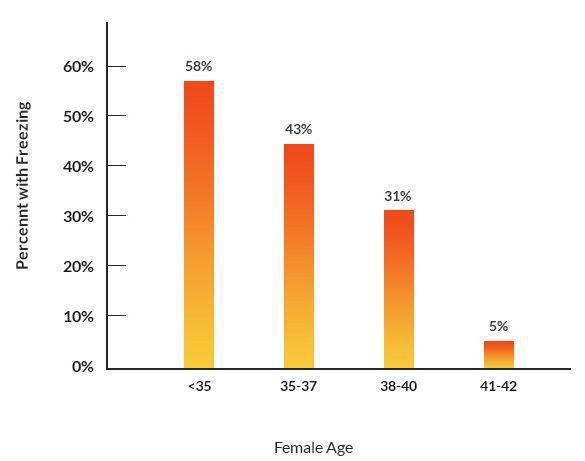
Percent of IVF egg retrievals with embryos frozen by female age
How many embryos are frozen on the average with an IVF cycle?
- This is also age dependent
- Younger women respond better to the IVF ovarian stimulation process and produce more eggs, resulting in a higher likelihood for having excess embryos available for freezing
- The graph below shows the average number of leftover embryos frozen in 2010-2011 according to the female’s age
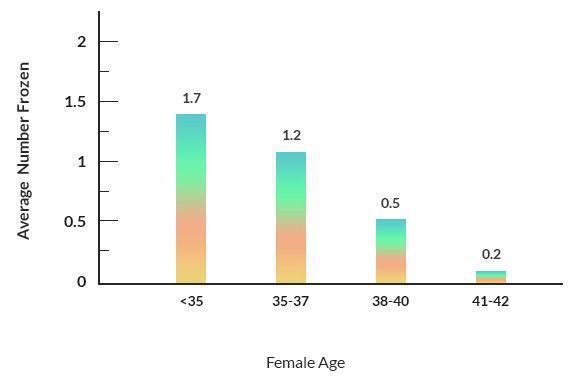
Average number of embryos frozen with IVF according to female age
What is vitrification for IVF?
- To embryologists, vitrification is ultra-rapid IVF embryo freezing instead of the traditional slow freezing process
- To a science dictionary, vitrification is the process of converting something into a glass-like solid that is free of any crystal formation
For example, by adding a cryoprotectant, water can be cooled until it hardens like glass without any ice crystals forming. This is important in the embryology world because ice crystal formation can be very damaging to frozen embryos (or other frozen cells).
Vitrification in IVF can allow freezing of spare embryos with better post-thaw survival rates and higher pregnancy and live birth rates from frozen embryo transfer cycles.
We started vitrification of blastocysts in our IVF lab in early 2008 and have seen excellent post-thaw embryo survival and substantially higher pregnancy rates after frozen transfer procedures.
A short history lesson
In 1972 preimplantation mammalian embryos were first successfully cryopreserved. The method was very time consuming. Slow cooling was used (1 degree/min or less) to about -80 degrees Centigrade. Then the embryos were placed in liquid nitrogen.
The embryos also needed to be thawed slowly and a cryoprotectant added and removed in many gradual steps. This was a lot of work.
The first reported pregnancy in humans from frozen embryos was in 1983.
Most of the research has been done on mouse embryos. Development of frozen thawed mouse embryos, in vitro and in vivo, is not statistically reduced as compared to their nonfrozen counterparts.
- This may now also be true for human embryos
- Research continues in this area and human embryo freezing and thawing protocols have improved tremendously over the past 25 years
- In some clinics (including ours), the newer vitrification technique is showing success rates for blastocyst embryos transferred after freezing and thawing that are equivalent to fresh blastocyst transfer success rates
Techniques for freezing eggs, sperm and embryos
Cryoprotectants are used in the solution that the embryos are frozen in. There are 2 basic types – permeating (e.g. propanediol) and non-permeating (or extracellular) such as sucrose.
Cryoprotectants are useful because they:
- Lower the freezing point and may prevent intracellular ice formation.
- May protect cells by interacting with membranes as they change from a pliable to a rigid state.
Embryos can be frozen at the pronuclear stage (one cell), or at any stage after that up to and including the blastocyst stage (5-7 days after fertilization). Different cryoprotectants and freezing solutions and protocols are used for different stages of embryo development.
- Many IVF clinics (including ours) are currently doing all of their embryo freezing at the blastocyst stage
- There has been a trend in the IVF world away from the traditional slow freezing method that has been used since the 1980’s
- Vitrification for IVF embryo freezing is becoming a much more widely used technique
Costs for embryo freezing, embryo storage and frozen embryo transfer cycles
- We charge $800 for cryopreservation (embryo freezing). We use the vitrification technique for embryo freezing (see above).
- Our IVF pricing page lists our current charges for storage of frozen embryos and also costs for a frozen embryo transfer cycle