Polycystic Ovarian Syndrome (PCOS) requires specific tests for diagnosis. How is the diagnosis of PCOS made?
What is Polycystic Ovarian Syndrome?
PCOS, short for polycystic ovarian syndrome, is a common cause of anovulation and female infertility. PCOS is also sometimes referred to as PCO (polycystic ovaries) or PCOD (polycystic ovarian disease).
- In 1935 doctors Stein and Leventhal first reported that polycystic ovaries were associated with lack of menstrual periods – amenorrhea.
- They described 7 women with amenorrhea, excess hair growth (hirsutism), obesity and enlarged ovaries.
- The women underwent surgery to have a “wedge resection” done on their ovaries.
- All seven resumed regular menstrual cycles after surgery
- Two of the woman conceived
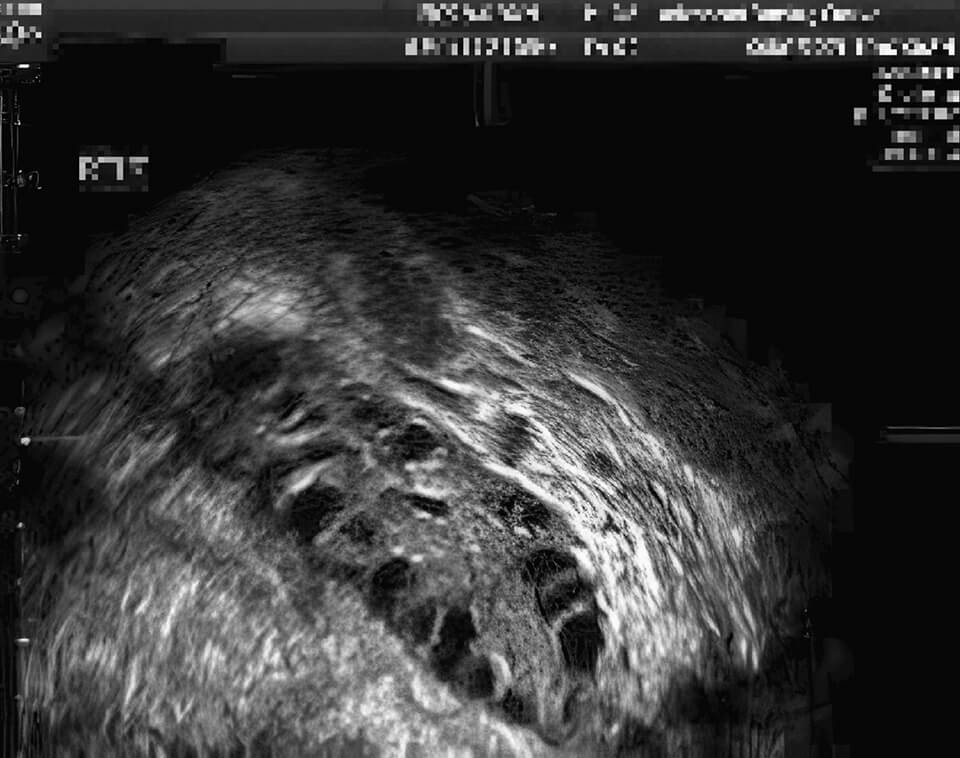
Ultrasound images: A polycystic ovary and a normal ovary
Polycystic ovary with many antral follicles
Normal ovary with a single mature follicle Yellow cursors are measuring the follicle

Features that can be seen with polycystic ovarian syndrome
- Irregular or absent menstrual cycles
- Evidence of excess male hormone (androgen excess)
- Hirsutism (excess male pattern hair growth), acne, enlarged clitoris (rare)
- Enlarged polycystic appearing ovaries by ultrasound
- Obesity
- Acanthosis nigricans (velvety,brown skin markings usually on the neck, under the arms or in the groin)
How do doctors make the diagnosis of PCOS?
Currently there is some disagreement among doctors about the criteria required in order to make the diagnosis of polycystic ovarian syndrome.
At least 2 definitions are commonly used:
- In 1990 a consensus workshop sponsored by the NIH said the diagnosis of PCOS can be made if all 3 of the following are present:
- Clinical or biochemical signs of androgen excess (high levels of male hormones)
- Oligoovulation (irregular or infrequent periods)
- Other entities have been excluded that would cause a polycystic ovary-like syndrome
- Another set of criteria for making the PCOS diagnosis is from the Rotterdam ESHRE/ASRM Sponsored PCOS Consensus. Workshop Group (2003). The diagnosis of PCOS can be made if 2 out of 3 of the following are present:
- Clinical or biochemical signs of androgen excess
- Oligoovulation (irregular or infrequent periods)
- Polycystic ovaries by ultrasound
- Other entities have been excluded that would cause a polycystic ovary-like syndrome
“Other entities” that need to be excluded would include:
- Congenital adrenal hyperplasia, a defect of the enzyme 21-hydroxylase. The hormone 17 hydroxyprogesterone (17-OHP) accumulates in the bloodstream in this condition.
- Cushing’s syndrome
- Androgen secreting tumor (very rare)
- Women with non-androgenic conditions such as hyperprolactinemia, that can result in irregular periods and polycystic ovaries.
What matters most is not what we name it, but whether we recognize the problem and treat it effectively.
What do we mean by “clinical or biochemical signs of androgen excess”?
Clinical observations are based on observed conditions that doctors find in the patients (including symptoms) – as distinguished from laboratory findings, such as results of blood tests.
Some clinical signs of androgen excess include:
- Hirsutism (excess male pattern hair growth)
- Acne
- Clitoromegaly – enlarged clitoris (rare)
Some biochemical signs of androgen excess include:
- Elevated serum testosterone (total testosterone)
- Elevated level of free testosterone
- Elevated dehydroepiandrosterone sulfate, also called DHEA sulphate, or DHEAS
Laboratory testing for patients suspected of having PCOS:
- Serum testosterone
- Prolactin
- 17-OH progesterone, 17 hydroxyprogesterone, 17 OHP
- LH, FSH, estradiol
- Dehydroepiandrosterone sulfate, DHEAS
- Thyroid stimulating hormone, TSH
Ready for an Appointment in the Chicago Area?
If you’re ready to explore treatment, contact the award-winning team at AFCC.
Find a Prelude Fertility Clinic Location Near You
The Prelude Network is the fastest-growing network of fertility centers in North America.
Diagnosing PCOS with Ultrasound
What does a polycystic ovary look like?
In a polycystic ovary, the numerous small cystic structures, also called antral follicles, give the ovaries a characteristic “polycystic” (many cysts) appearance on ultrasound (see images at top of page).
The older literature on ultrasound evaluation and diagnosis of “polycystic ovaries”required that:
- At least one ovary is greater than 10 cm³ in volume
– or – - At least one ovary has 12 or more antral follicles seen by ultrasound
- However, in my opinion this is outdated. Ultrasound equipment has improved and we currently see more antral follicles than we did in the past.
- In our practice, patients with polycystic ovarian syndrome generally have 40 to 100 antral follicles (total).
- I would generally not be considering a diagnosis of PCOS if the woman has less than a total of 30 antral follicles (sum of counts from both ovaries).
Diagnosing PCOS with FSH and LH Hormone Levels
Many (but not all) women with PCOS have an abnormal FSH to LH ratio.
In order for proper follicle and egg development to proceed, FSH (follicle stimulating hormone) and LH (luteinizing hormone) each need to be present at certain levels and at specific times during the normal menstrual cycle.
- Normally this ratio is about 1:1 – meaning the FSH and LH levels in the blood are similar.
- FSH and LH are often both in the range of about 4-8 in young fertile women.
- In women with polycystic ovaries the LH to FSH ratio is often higher – for example 2:1, or even 3:1.
- With PCOS we often see the FSH in the range of about 4-8 as well – but often the LH levels are 10-20.
- It is common for women that clearly fit the PCOS syndrome in other ways to have normal serum FSH and LH levels and a normal FSH to LH ratio.
- For this reason, testing of FSH and LH hormone levels is not always helpful when trying to diagnose PCOS.