
How to get pregnant after your tubes are tied
Tubal reversal surgery or IVF, in vitro fertilization, after tubal ligation
Bundled price for tubal reversal of $9,000, including our fees, the surgery center and anesthesia
Women who have had tubal ligations sometimes regret their decision and desire fertility in the future. There are 2 options for fertility after tubal ligation, tubal reversal surgery and in vitro fertilization - IVF. Both of these are reasonable options and how the woman chooses to proceed should be based on an educated consideration of the pros and cons of each.
Most women have their tubes tied before they leave the hospital after they deliver a baby, or they come in for tubal ligation by laparoscopy which is an outpatient surgical procedure done through a scope that goes through the belly button.
Tubal reversal surgery usually requires a laparotomy which is a much larger incision on the abdomen usually approximately 4 to 6 inches in length. Since the skin and all the muscles and other tissues of the abdominal wall must be cut through there is considerably more discomfort and a much longer recovery time following the surgery as compared to a laparoscopic surgery such as with a tubal ligation.
Some surgeons are now performing tubal reversal surgeries through the laparoscope. However, this is a relatively difficult technique and there is not yet sufficient published data to know what pregnancy rates will be after laparoscopic tubal reversal.
Most women will need to be in the hospital for approximately 3 days following tubal reversal surgery and will need to be off work for a minimum of 2 to 3 weeks.
There are 5 important issues regarding tubal reversal surgery that need to be considered and discussed. The sperm quality of the male partner, tubal status, status of other possible pelvic conditions, female age, and egg quantity and quality. Sperm quality
The male partner needs a sperm test prior to decision making about tubal reversal vs. IVF after tubal ligation. If the sperm quality is good, then the couple could possibly consider both options. If the sperm quality is poor, in vitro fertilization is the better option. This is because pregnancy rates are low without using in vitro fertilization if there is poor sperm quality (low sperm count or motility). With IVF with ICSI, poor sperm quality is easily overcome.
Tubal status
The length of the remaining tubal stumps after tubal ligation (or cauterization if the tubes were burned instead of tied or clipped) is very important. The longer the 2 remaining stumps are on each side the better the chances for successful reversal and pregnancy. The shorter the stumps the lower are the chances for pregnancy.
Unfortunately, it can not be known how much tube is remaining for certain without surgery. A hysterosalpingogram (dye test in radiology) can tell us how long the proximal stump is (the piece of tube attached to the uterus) but the dye test will not tell us anything about the length of the distal stump (the far end of the tube that has been separated from the uterus).
Some women go through tubal reversal surgery with very short tubes. This results in low chances for subsequent pregnancy.
The fimbria are delicate, fluffy structures at the end of the tube that "pick up" the egg when it is released from the ovary at the time of ovulation. If the fimbriated end of the tube is damaged or has been removed, chances for success with reversal are low.
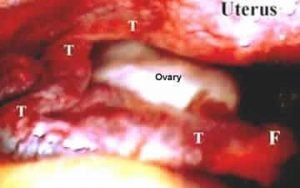
Laparoscopy picture showing delicate fimbria (F) at end of normal fallopian tube (T),the fimbria are close to the ovary so it can pick up the egg at ovulation
If both portions of fallopian tube are significant long (sometimes they are quite short), the fimbria are in good condition, and the surgery is done expertly, the expected pregnancy rate in young women (under 35) without other fertility problems (male partner also has good sperm quality) should be about 75%.
This means that after 1 year of trying 75% of women should be able to get pregnant if the tubal anatomy was good and these other factors are all normal. If any of these factors are abnormal, expected pregnancy rates after tubal reversal would be significantly lower.
Ready for an Appointment in the Chicago Area?
If you’re ready to explore treatment, contact the award-winning team at AFCC.
Find a Prelude Fertility Clinic Location Near You
The Prelude Network is the fastest-growing network of fertility centers in North America.
Status of any other pelvic conditions
Pelvic endometriosis or any scar tissue in the area of the tubes or ovaries would be expected to reduce the chances for success after tubal reversal surgery. However, IVF pregnancy success rates are generally not affected by these conditions. Therefore, in vitro fertilization is probably a better option in women with significant endometriosis or pelvic scar tissue.
Female age
Chances for pregnancy with either tubal reversal or IVF decline in the mid to late 30's and more dramatically starting at about age 38. By age 43-44, very few women will be able to have a baby using either approach. This issue makes careful and honest counseling very important for women between about 35 to 43 years of age.
I would discourage women 43 and older from pursuing either option because of the dismal success rates at that age and beyond. Egg donation is a more viable option iat that age.
Egg quantity and quality
Some women have a decline in either egg quantity or quality earlier in life than expected. Therefore, the woman's "ovarian reserve" should be tested before a decision is made regarding whether to proceed with either tubal reversal or in vitro fertilization. Ovarian reserve is usually assessed by an ovarian antral follicle count, ovarian volumes and day 3 FSH levels.
Tubal reversal surgery
The biggest advantage of tubal reversal surgery over IVF is that once the women has gone through the surgery she hopefully will not need any intervention through a physician such as drugs, medications or procedures in order to get pregnant. Obviously, the idea is that good old fashion sex will then give them the baby that they want.
There is also very low risk for multiple pregnancy - twins occur naturally in only 1 in 90 pregnancies. The biggest disadvantage is the fact that the women has to go through a big surgery and if pregnancy does not result after the tubal reversal her only option remaining is in vitro fertilization.
A small disadvantage is that after she has her additional child (or children), she will need to use contraception or have her tubes (or her male partners) tied again.
In vitro fertilization - IVF
In vitro fertilization involves stimulating the woman with medications, taking a number of eggs from her ovaries, fertilizing them with her male partners sperm and transferring some of the resulting embryos back into her uterus with the hope that one will implant. There is detailed information elsewhere on this site about in vitro fertilization.
The biggest advantage of in vitro fertilization is that the woman can avoid avoids the major surgery involved with a tubal reversal. Another advantage is that the outcome is known 10 days after the procedure when we do the first pregnancy test rather then waiting for a year or more to find out whether the procedure is successful.
Success rates with IVF vary greatly according to the program. Some IVF programs have pregnancy rates with tubal factor infertility of over 50% per attempt in women under 40 years old. Other programs with the same type of patients report pregnancy rates of only 20 to 30% (or sometimes less).
The reason for this is that some in vitro fertilization programs are better than others. This is why the couple should do careful comparisons of in vitro fertilization success rates before choosing an IVF specialist and clinic.
The biggest disadvantages of in vitro fertilization are that the woman has to take medications to stimulate development of multiple eggs and that there is always some risk for multiple pregnancy.
The biggest disadvantages of in vitro fertilization are that the woman has to take medications to stimulate development of multiple eggs and that there is always some risk for multiple pregnancy.
However, multiple birth risks can be controlled by limiting the numbers of embryos transferred to 1 (or 2). Another disadvantage is that if the first attempt does not work the couple must do IVF again. Often there would be left over embryos that were frozen from the first cycle - it is much less expensive and easier for a second attempt using the frozen embryos. However, if there are not any frozen embryos, the cost for the second attempt is usually the same as for the first one.
Costs for tubal reversal surgery and IVF costs
Physician charges for tubal reversal surgery and for IVF vary greatly across the country. Most physicians charge a professional fee of somewhere between $3000 and $8,000 for the tubal reversal surgery. On top of this will be hospital charges which are usually between $7,000 and $20,000. Insurance will rarely pay any of these charges.
- We have a bundled price for tubal reversal of $9,000 - includes our fees, surgery center and anesthesia
IVF costs between about $7,000 and $17,000 plus medications depending on the program. Medication costs vary according to the amount needed for the individual woman, but average about $2500 - $3000 for the cycle.
- Our IVF cycle package cost is $10,000 plus medications
- We also offer a multiple cycle IVF plan and a money-back guarantee IVF pricing option
There is no correlation between the price programs charge and the pregnancy success rate. Some of the most expensive programs have very low pregnancy rates and some of the lower cost programs have very high pregnancy rates. "You get what you pay for" does not necessarily apply for in vitro fertilization.
| What's involved | Expected pregnancy rate | Tubal pregnancy rate | |
|---|---|---|---|
| Tubal reversal | Surgery, abdominal incision, 1-3 weeks recovery time | 40-75% over 1-2 years (age under 35) | 5-15% of pregnancies |
| IVF after tubal ligation | Shots for about 10 daysEgg retrievalEmbryo transfer | 60-70% for one cycle (at our clinic, age under 35) Our IVF Success Rates | 1% of pregnancies |
Women that have had tubal ligations often ask us:
"What is the best way for me to have another baby, should I do IVF or should I have the tubal reversal surgery?"
I do not believe that there is a "best" way. The best way to try to have another baby for an individual woman is up to her. She needs to learn about the pros and cons of both approaches and then consider risks, benefits and costs involved with each one.
Having said all of this, very few women come in asking for reversal surgery anymore. They almost always have read about both options and want in vitro fertilization. The OB/GYN physicians are most often telling them to go for IVF as well. If we had a crystal ball that would tell us what, if anything, would get the couple a baby it would be easy to decide.
If anyone has such a crystal ball for sale, please call me immediately. I will pay very well for it...
For more information about details regarding tubal reversal surgery and IVF, there are many other pages on this website related to both tubal surgery and in vitro fertilization.
Categories
About the AFCC Blog
Welcome to the Advanced Fertility Center of Chicago’s blog! Here, you will find information on the latest advancements in fertility care and treatments, including IVF, IUI, third-party reproduction, LGBTQ+ family building, preimplantation genetic testing, and more. Since 1997, we’ve used our experience and continuous investment in the latest fertility technology to help thousands of patients grow their families. Contact us today for more information or to schedule a new patient appointment.